Maternal spindle transfer is a complex fertility method that prevents the inheritance of mitochondrial diseases. Since it requires the genetic material of three people, it raises ethical questions, with some voices arguing that it could open the door to producing designer babies. While legislation in many countries prohibits the manipulation of embryos, laws often allow practices that have a therapeutic purpose. 2017 AsiaGlobal Fellow Florencia Daud, a lawyer who specializes in bioethics and in-vitro fertilization, discusses the limits and dilemmas of the treatment.
In-vitro fertilization: Since maternal spindle transfer requires the genetic material of three people, it raises ethical questions, with some voices arguing that it could open the door to producing designer babies (Credit: posteriori / Shutterstock.com)
On September 23, 2021, South America’s first three-parent baby was born. She was conceived using maternal spindle transfer, a fertility method that uses the genetic material of three people. The treatment was carried out at PROCREARTE, a fertility center based in Buenos Aires – one of few laboratories around the world that have successfully executed the complex procedure.
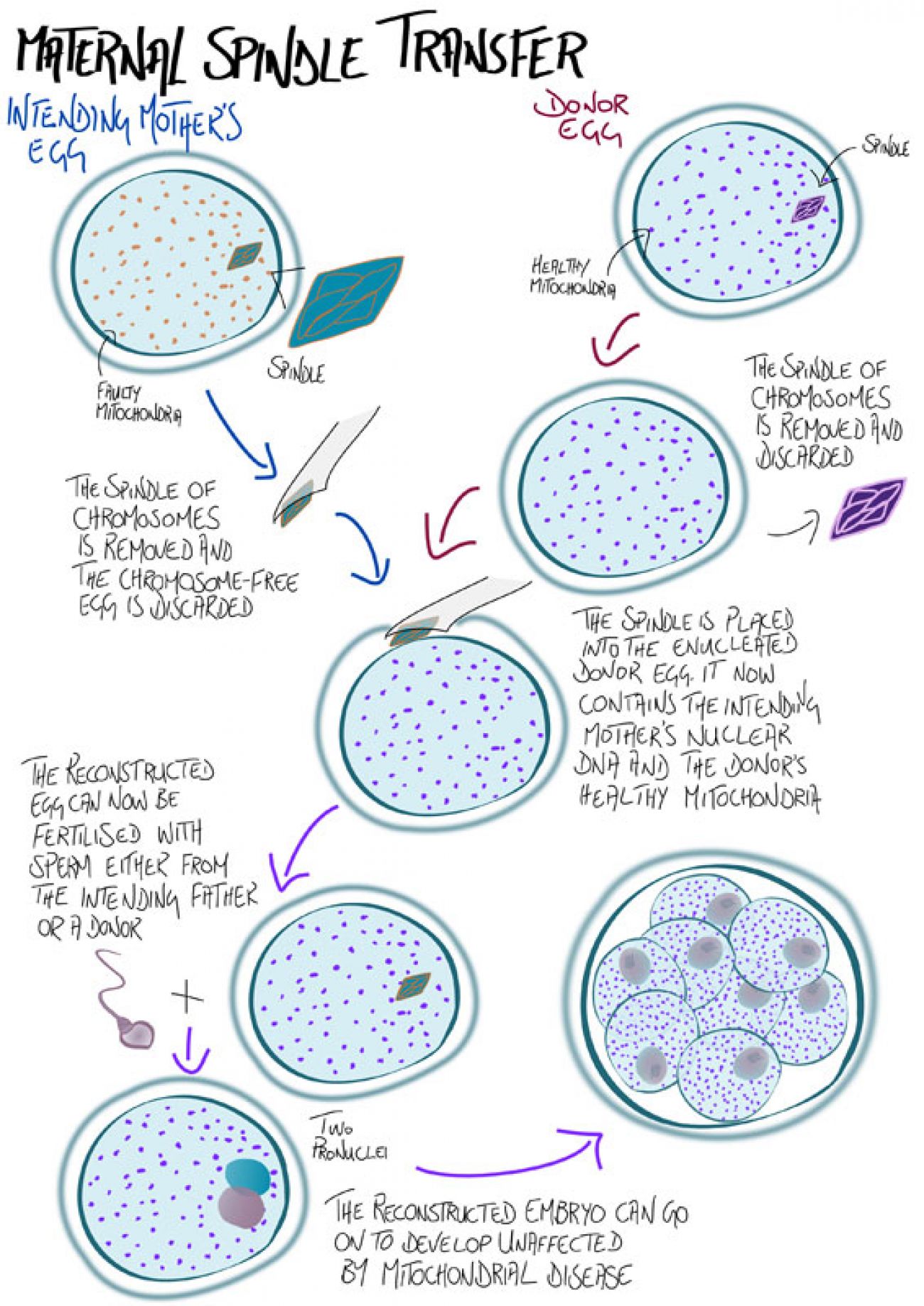
Maternal spindle transfer involves extracting the nucleus or meiotic spindle – a major structure involved in the production of sex cells – from the oocyte (immature egg cell) of a patient carrying mitochondrial DNA mutations, and transferring it to the cytoplasm of an enucleated donor oocyte with healthy mitochondria. This reconstituted oocyte, when fertilized, produces pregnancy without the inheritance of mitochondrial diseases – metabolic disorders which could affect organs or tissues such as the brain, heart, liver and kidneys.
Although maternal spindle transfer was developed to prevent mitochondrial diseases, its indications have been extended to healthy patients but with repeated implantation failures, offering an alternative to those who must resort to egg donation. In the case of the first baby born in Greece in 2019 through a maternal spindle transfer, the mother had a low ovarian response and the process was sought as a solution to infertility.
Because human cells, not embryos, are manipulated during maternal spindle transfer, the process is not necessarily controversial. But as scientific studies indicate, we are conditioned by nongenetic components in the ova from which we are born.
Based on these findings, the development of a person who is born through this new technique will be influenced by three people. We must remain cautious, since the technique is new and unforeseen consequences could be transmitted to future generations. Some voices also argue that the technique opens the door to the production of superior offspring.
Legal considerations across the globe
In 2017, the first maternal spindle transfer was performed by Dr John Zhang, founder of New Hope Fertility Center in New York City, and a team of North American scientists. Since the procedure is not allowed in the US, the zygote was created in New York and the transfer was done in Mexico City. The lack of regulation in the country made the birth possible. In Ukraine and Greece, mitochondrial substitutions have also been carried out. The United Kingdom even pioneered the authorization of mitochondrial replacement through legislation in 2015.
Genetic alterations to the germ line – the lineage of cells that eventually forms eggs and sperm in adults – are prohibited in most countries to protect the genetic pattern of humanity, the right to an unmodified genome and information about genetic identity. Modifying reproductive cells (ovules, sperm or embryos) may result in undesirable consequences for both the unborn child and their offspring. Maternal spindle transfer leads us to rethink the limits of this prohibition and the rationale of these treatments. Because this technique new, few countries have laws to govern it.
In the case of Artavia Murillo et al v Costa Rica, the Inter-American Court of Human Rights ruled that the existence of the human person begins with the implantation of the embryo. According to this criterion, the sex selection of embryos in assisted reproduction is allowed and the selection of embryos made in preimplantation diagnostic tests, during which embryos with alterations are discarded, is permissible.
Since mitochondrial DNA is inherited maternally from the mitochondria present in the egg, girls born through maternal spindle transfer would pass the donated mitochondria to their own children, making the genetic change heritable. The same cannot be said for males. Therefore, only by using male embryos can we prevent germ-line changes from passing to future generations.
Recommendation 934/82 of the Council of Europe addresses the intangibility of the genetic inheritance of humanity and proposes to include it on the list of human rights to protect it from the artificial intervention of science or technology. The European Parliament Resolution on the Ethical and Legal problems of genetic manipulation has also referred to this issue. In articles 27 and 28, it calls for the prohibition of attempts to genetically reprogram human beings and the criminalization of any transfer of genes to human germ cells.
The Convention on Human Rights and Biomedicine, which is a “legally-binding international text that aims to preserve human dignity, rights and freedoms”, states in Article 13 that only genetic intervention that is preventive, diagnostic or therapeutic and does not have the objective of modifying the genome of the offspring should be allowed. Article 6 of the UNESCO Declaration on the Responsibility of the Present Generations Towards Future Generations, adopted on November 12, 1997, expresses the need to preserve biological diversity and to protect the human genome by virtue of human dignity and human rights.
The legally binding nature of these documents could cause problems. For example, Article 26.2 of the Convention on Human Rights and Biomedicine clarifies that Article 13 cannot be restricted by the state. In turn, Point 91 of the Convention’s Explanatory Report states, “Interventions that try to introduce any modification in the genome of the descendants are prohibited. Thus, the modification of sperm or ovules for fertilization is not particularly allowed”.
It must be taken into consideration that modifying mitochondrial DNA is not the same as nuclear DNA. While the latter determines the essential traits of our personality, mitochondrial DNA could never cause that effect. Legally, it is possible to differentiate between the alteration of one from the other. It is not entirely clear, however, if mitochondrial substitution, a key component of maternal spindle transfer, can be excluded from Article 13. If mitochondrial replacement techniques are included, according to Article 38 of the Convention, legalizing it in signatory countries would require a reform or denunciation of the Convention.
Can mitochondrial replacement techniques be considered genetic modification in a strict sense? If so, should they be considered germinal, and therefore heritable? If only male embryos were implanted to prevent germ-line changes from passing to future generations, mitochondrial replacement should be considered somatic gene therapy as changes would not be heritable and would stop with the male donor, who would not be able to transfer mitochondrial DNA.
Taking into account that there are countries such as Spain where the selection of the sex of the embryos is forbidden, these issues should be carefully evaluated.
If “modification” is defined as any intervention or change in the genetic material contained in a cell, even the act of transferring it from one place to another without changing its DNA sequence would be an act of modification, according to the Convention. But, since “modification” is understood as interventions to modify a DNA sequence – nuclear or mitochondrial – through the introduction, deletion or modification of genes, maternal spindle transfer would not fall into that category as the process keeps both nuclear DNA and mitochondrial DNA intact.
Article 13 of the Convention authorizes the modification of human genome for preventive, diagnostic or therapeutic reasons, only when the purpose is not to introduce any modification in the genome of descendants. The article would apply to maternal spindle transfer if “descendants” refer to the children born as a result of the treatment, but if what is being prohibited is the introduction of modifications to the germ line that can be transmitted to subsequent generations, it would only be prohibited in relation to female embryo transfer as transferred male embryos would not pass unwanted side effects to future generations.
There is now an intense debate in Australia around the approval of a bill that would allow mitochondrial donation. One of the arguments against the bill is egg donation can safely prevent the transfer of mitochondrial disease from mother to child. This, however, means the mother would not be able to pass on her genes.
The Australian model resembles the United Kingdom’s dual license system. In Australia, only one clinic would be licensed to offer mitochondrial donation during the first phase, which is expected to last 10 to 12 years. Every patient who wishes to undergo the procedure will also need separate approval and be subject to eligibility requirements that are similar to those in the UK.
One major difference between the two models is the right to information on donor identification data: in Australia, this right would be extended to children born by mitochondrial donation, while in the UK, mitochondria donors can remain anonymous. The UK allows anonymity because they would contribute less than 1 percent to the child’s genetics. In both countries, children born after in vitro fertilization with egg or sperm donation have the legal right to obtain identifying information from their donors upon reaching the age of majority.
The UK rejected the possibility of choosing only to transfer male embryos, but, in Australia a third alternative was proposed: to let the parents decide whether to transfer a male embryo or proceed without sex selection. This intermediate proposal does not resolve ethical questions about sex selection. Also, even if parents receive counseling, they may not be equipped to make well-informed decisions.
Current dilemmas
Genetic identity makes human beings unique. Reproductive cloning involves replicating nuclear genetic identity. Given that mitochondrial substitution requires nuclear transfer to be carried out, it is important to analyze whether it contradicts international regulations on reproductive cloning, such as Article 11 of the Universal Declaration on the Human Genome and Human Rights (November 11, 1997), the Additional Protocol to the Convention of Human Rights and Biomedicine on the Prohibition of Cloning Human Beings (November 6, 1997), and article 3.2 of the Charter of Fundamental Rights of the European Union (December 7, 2000). It would seem that it does not: Persons born from mitochondrial substitution will not share the same nuclear genetic map as another human being, whether they are living or dead.
On the other hand, with regard to the concern over whether persons born by meiotic spindle transfer would develop some sort of identity crisis, it is worth noting that the presence of third-party DNA is already common in heterologous assisted fertility in the cases where the donation of male or female gametes, or both, are used.
During the debates in Australia, it was argued that the Mitochondrial Replacement Bill would open the door to ethically questionable practices. In principle, it would make it legal to produce and destroy embryos until a viable one is achieved for implantation. The practice would otherwise be prohibited in the country.
The interest in non-modification is centered on avoiding the selection of human beings. But taking into consideration the entire human species, it does not seem that the meiotic spindle transfer can be generalized on a scale of the magnitude necessary to produce an effect on the evolutionary process. The Australian Senate passed the bill at the end of March, the last hurdle for what is known as Maeve’s Law after Maeve Hood, a girl who inspired the legislation, to be adopted.
To make ethical judgments and legal decisions, it is necessary to weigh the different degrees of modification to genetic integrity produced by each of these techniques. There is a difference between genetic alterations that have therapeutic purposes, as opposed to determining physical, psychological or personality traits. Since the transfer of the meiotic spindle does not influence physical or personality, it would seem that ethical and legal objections are lower.
Other types of questions that arise include how countries should allocate funds from the health budget. If only those who can afford to pay for medical insurance had access to this new technique, the principle of equality would be broken, causing even more inequality by guaranteeing access to genomic techniques to high-income individuals.
Another question is how donor eggs should be obtained. They could be drawn from the existing pool of donated eggs for assisted fertility treatments, but that would mean that current egg donors may not have anticipated that their eggs would be used for mitochondrial donation and therefore have not specifically consented to that use. Eggs should be obtained from donors who have given specific consent.
If the benefits that are obtained through meiotic spindle transfer are bigger than the risks, it is likely that doctors and patients will continue using it. From current international regulations, it can be inferred that the transfer of the meiotic spindle is not completely prohibited, since the practice can be carried out in countries with more ambiguous regulations. As biologists, doctors and laboratories around the world may be qualified to execute such a procedure, specific regulations to govern the procedure would be necessary in most countries.
Further reading:
Asia Global Institute
The University of Hong Kong
Room 326-348, Main Building
Pokfulam, Hong Kong
asiaglobalonline@hku.hk
+852 3917 1297
+852 3917 1277
©2026 AsiaGlobal Online Journal
All rights reserved. Terms of Use - Privacy Policy.
Opinions expressed in pieces published by AsiaGlobal Online reflect those of the authors and do not necessarily represent the views of AsiaGlobal Online or the Asia Global Institute.
The publication of AsiaGlobal Voices summaries does not indicate any endorsement by the Asia Global Institute or AsiaGlobal Online of the opinions expressed in them.

Check out here for more research and analysis from Asian perspectives.